CNN reports on the way that my own Obamacare expenses (my premiums plus deductible for next year will be close to 40 percent of my 2015 adjusted gross income) are not unusual.
“These costs are largely a symptom of the fact that medical costs in this country are extraordinarily high,” said Kevin Counihan, CEO of the federal exchange, healthcare.gov. “We have an 800-lb gorilla here, which is exploding health care costs.”
1. Regardless of what economic theory suggests about health care policy, the political system is heavily biased toward stimulating demand while restricting supply. For example, Obamacare stimulated the demand for health insurance through a combination of mandates and subsidies, and yet it restricted supply in that it gave consumers fewer choices. Hence, the “exploding health care costs.”
However, this political bias has operated much more broadly and for much longer. Medicare and Medicaid stimulated demand, while supply has been tightened by restrictions on medical licensing, practice regulation, and regulatory limits on hospital construction.
The most economically beneficial reforms of health care would run counter to this political bias. That is, they would serve to increase supply and cut back on the stimulus to demand. Of course, such reforms are not going to be popular politically.
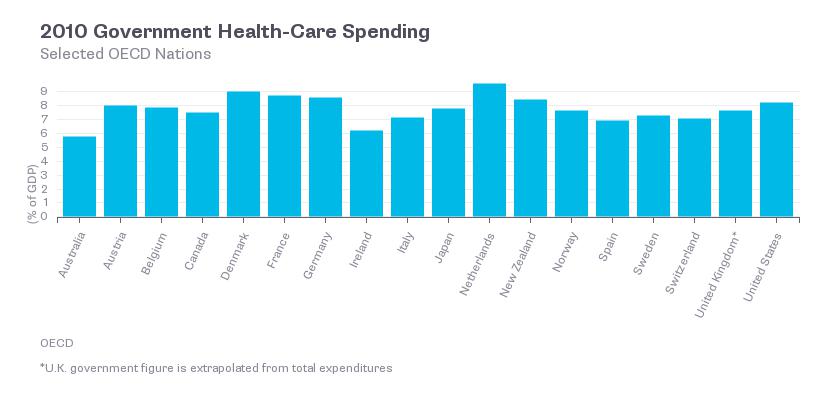
2. The hope that a single-payer system will reduce costs is misplaced. Compared to what many major industrial countries spend on health care, we spend a higher proportion of our GDP on Medicare alone. [UPDATE: a commenter pointed out that I need to include Medicaid. In fact, I also need to include government employee benefits. See the table from the OECD which is found in this piece by Megan McArdle. As I pointed out ten years ago in Crisis of Abundance, our high spending reflects a willingness to undertake a lot of medical procedures with high costs and low benefits.
3. As individuals, each of us would like unlimited access to medical services without having to pay for them. Collectively, we cannot afford this, because it leads to over-utilization and waste. As our rate of health care spending becomes unsustainable, we are going to get a combination of third-party rationing (denial of coverage for some medical services in some situations) and self-rationing (insured individuals facing higher deductibles and co-pays will choose not to obtain some medical services). If the left has political control over health care policy over the next ten years, I expect to see more third-party rationing. If the right has political control over health care policy over the next ten years, I expect to see more self-rationing.
4. A two-tier health care system is all but unavoidable. If the government provides basic health care for all, then the rich will go outside the system for expensive procedures. For example, Canadians can come to this country for treatments that they cannot obtain in Canada. If the government limits its involvement to providing health care vouchers to poor people, then they will not be able to afford the services that the rich are able to obtain.
5. New discoveries in health care tend to make existing programs and policies anachronistic. The FDA is often a roadblock to innovation. Medicare and Social Security have not adapted to greater longevity. Incentives for innovation are too dependent on the patent system, as opposed to prizes or other methods. New forms of health insurance, such as “insurance against becoming uninsurable,” need to be tested in the market.
{kind=link}